Difference between revisions of "Broken/1/OrthoNeuroGnatodontics"
Rosa.simao (talk | contribs) m (1 revision imported) |
m (1 revision imported) |
(No difference)
| |
Latest revision as of 13:13, 19 February 2022
OrthoNeuroGnatodontics on 2° Class patient
OrthoNeuroGnatodontic treatment on 2° Class patient, ipodivergente con Deep Bite
Presentation
12-year-old patient who shows to the cephalometric examination, a underdevelopment of the jaw, which is small and not very projected, and imprisoned in the maxilla. The hypodivergent growth also determines a severe deep bite that does not allow the eruption of the upper canines in the presence of class 2 molar. The trigeminal electrophysiological tests (not reported here) ensured that the patient, in the conditions in which he presented himself for the Ortho-NeuroGnathodontic treatment, was in a State of System Coherence such that the occlusal imperfection could be corrected through classic orthodontic masticatory rehabilitation. If the electrophysiological responses had shown neuromotor discrepancies, a State of system decoherence would have been added to the occlusal imperfection to be treated with functional neuro-gnathological therapies to restore the state of System integrity (Figures 1, 2 and 3)
The cephalometric analysis showed a skeletal Class 2 morphology, hypodivergent, biretrusive profile with SNA 80 °, SNB 75 ° and ANB 5 °.

Figure 1: Patient’s Right side view

Figure 2: Patient’s Front side view

Figure 3: Patient’s Left side view



Treatment/Operation
The 1st phase of the treatment consisted in restoring the maxillary spaces and volumes through molar distalization by means of NiTi Opencoil (nickel titanium open spring) between the first premolars and the molars which allows to obtain in addition to the recovery of the 1st molar class also the recovery on the sagittal plane of the space necessary for the canines. The use of class 2 elastics is essential to avoid the mesializing counter vector on the upper frontal group, as well as the lip bumper inserted in the tubes of the bands in the lower molars avoids the mesializing component on the lower arch through the lip thrust on the resin shield. (Figure 4)

Figure 4: Lateral aspect of the 1st phase of OrthoNeuroGnathodontics treatment
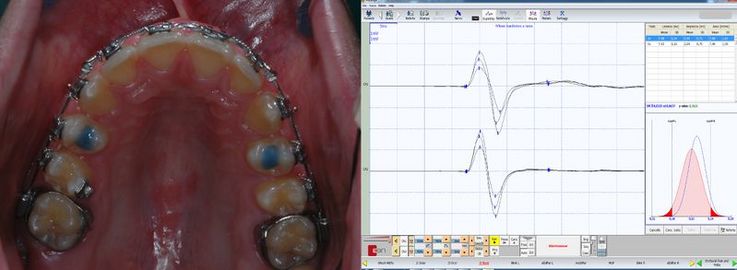
Figura 5: Left view of the occlusal raisebite on 14 and 24 performed with the aid of trigeminal electrophysiology (image on the right side) and in particular through analysis of the jaw jerk. The upper trace indicates the right masseter.

Figura 6: Right, front and left side view of the case being finalized
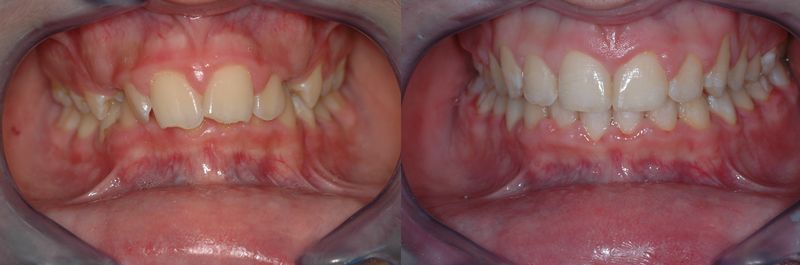
Figura 7: View of the pre and post treatment clinical case
_-_1st_phase_of_OrthoNeuroGnatodontic_treatment_(001).jpg)
.jpg)
.jpg.jpg)
_-_facial_hypodivergent_morphology,_OrtoNeuroGnathodontics.jpg)
Follow up
Finalization of the clinical case with stabilization of the increased Occlusal Vertical Dimension and of the Centric Occlusal
In this phase it is absolutely important to check the alignment torque and the occlusal asymmetries in order not to generate an incisal anterior wall and occlusal interference which, in increase of the Occlusal Vertical Dimension, could increase the spatial error in the intermaxillary relationship. As reported in the introduction of Masticationpedia, the evaluation of the Central Nervous and Peripheral Trigeminal System is a keystone to interpret the Masticatory System as a Complex System and guarantee or at least reduce the incidence of iatrogenic damage from treatment such as rrelapses. Figure 7 shows the success of Orthodontic Aesthetic Follow up 5 years: the occlusal aesthetic result is optimal and there are no relapses. This clinical result is not only due to a classic and careful orthodontic procedure, but also to the occlusal stability which does not generate interference or cleavage plans which can determine pairs of twisting forces on the teeth and even more seriously at the level of the Temporomandibular Joints. In Figure 8 we can see, in fact, the perfect symmetry of the jaw jerk and the Mechanical Silent Period. These trigeminal electrophysiological steps will be extensively exposed and discussed during the implementation of Masticationpedia while in this context they should only be considered in a demonstrative way. Note, in addition to the aesthetic of the smile, the perfect symmetry of amplitude of the jaw jerk (Figures 8, 9 and 10)
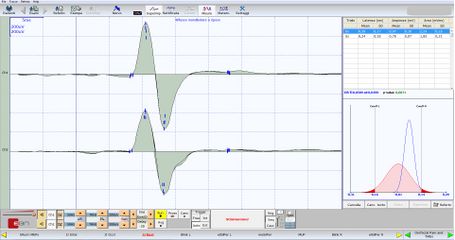
Figure 8: Clinical case concluded and at 5 years of following. Note the perfect amplitude symmetry of the jaw jerk

Figure 9: Clinical case completed and results at 5 years of following. The occlusal stability depends on the Coherence between the Neuromotor Systems
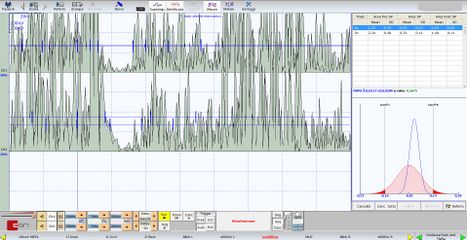
Figure 10: Clinical case completed and results at 5 years of following. Please note the perfect size symmetry of the integral area of the masseteric silent periods



![]() Book Index
Book Index
Next contents:
- Logic of medical language
- Classical logic
- Probabilistic logic
- Fuzzy logic
- System logic
- 1st Clinical Case: Emimasticatory spasm
- Complex Systems
- Coherence and decoherence
- Conclusive considerations
- Status quo and Criticity
- 2rd Clinical Case: Pineal Cavernoma
- Conclusions
- Status quo and Criticity
- 3th Clinical Case: Meningioma
- Conclusions
- Status quo and Criticity
- 4th Clinical Case: Eaton Lambert myasthenia
- 5th Clinical Case: Postpoly syndrome
- 6th Clinical Case: Temporomandibular disorders
- Conclusions
- Status quo and Criticity
- 7th Clinical Case: glioblastoma of the cranial base
- Conclusions
- Definition of the Fundamental Unit
- Structural and functional connectivity Separation
- Understanding of "Emergent Behavior"
- Connectivity measurement
- System Stochasticity
- Markov chains
- Inference of nonlinear Markov processes
- Understanding of Network nodes
- Center of the Masticatory Pattern
- Mesencephalic mechanisms
- Trigeminal Motor nucleus
- Proprioceptive mechanisms
- Neuromuscular spindles
- Sensory mechanisms from the depressor muscles
- Golgi Tendon Organs
- Role of impulses from the neck muscles
- Periodontal and Oral Sensory Factors
- Pharyngeal sensory factors
- Reflex of mandibular closure
- Sensory factors of the TMJ
- information transferred over time
- System Coherence Recovery
- 8th Clinical Case: Coherence Recovery in ort Orthognathic
- Sensitivity, Specificity and Predictive Values
- Advantages and limitations of the RDC
- Jaw opening width
- Speed of mandibular movement
- Complexity of chewing kinematics
- Computerized Tomography of the TMJ
- Magnetic resonance imaging of the TMJM
- Advantages and limits of pantography
- Pantographic Reproducibility Index
- Advantages and limits of axiography
- Advantages and limits of the electrognatography
- Free way space before stimulation
- Free way space after stimulation
- Closing trajectory from TENS
- Interferential EMG
- EMG at rest position
- Quantitative analysis of the EMG
- Fourier transform
- Wavelett
- Trigemnal electrophysiology
- Trigeminal electrophysiological segmentation
- Electric Motors Evoked Potentials
- Magnetic Motors Evoked Potentials
- Jaw jerk reflex
- M-wave
- Masseteric Mechanical Silent Period
- Masseteric Electric Silent Period
- Masseteric Laser Silent Period
- Recovery Cycle of Masseteric Inhibitory reflex
- Definition of the Fundamental Unit
- Maximal Neuronal Energy Evoked
- Organic motor symmetry
- Functional motor symmetry
- Renormalization
- Separation of structural and functional connectivity
- Organic vs Functional Symmetry
- Functional Neuro Gnathological Index "NGF"
- Organic vs Functional Symmetry
- New paradigm in masticatory rehabilitations
- Prosthetics
- Implantoprosthetics
- Orthodontics
- Orthognatics