Temporomandibular Joint
The DRC has tried to establish some clinical and laboratory references for the diagnosis of ATM disorders called DTM and tissue degeneration such as arthritic, remodeling forms, etc. but, before entering into the more in-depth discussion of TMJ imaging diagnostics, it is good to introduce some general aspects:
According to Priscila Brenner Hilgenberg-Sydney's article,[1] temporomandibular disorder (TMD) is an umbrella term encompassing conditions involving the temporomandibular joint (TMJ), masticatory muscles and/or associated structures.[2] Disc dislocation, TMJ sounds, congenital malformation, degenerative joint disease (DJD) are possible conditions affecting the TMJ. DJD is characterized by hard and soft tissue deterioration and abrasion of the TMJ and concomitant remodeling of the underlying subchondral bone. DJD has a multifactorial aetiology that has certain risk factors such as age, genetics, trauma, muscle or joint disorders, and systemic conditions. Clinical symptoms may include pain, joint noises such as crepitus, joint stiffness and/or restriction of jaw movement.[3]
Much effort has been made in recent years to develop standardized criteria for the diagnosis of TMD. The Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD), is a widely used research protocol to evaluate TMD. A revised version was published as Diagnostic Criteria (DC/TMD) in 2014, with the aim of being feasible for clinicians as well. In the first validation paper, TMJ imaging was optional for diagnostics, while the second recommends it for proper evaluation.[4]
Nowadays, there are many imaging modalities to investigate TMJ, such as CT, cone-beam CT (CBCT), MRI, plain radiography, ultrasound, pantomograph (commonly called "panoramic "), arthrography, among others.[5] The literature is still unclear when a patient with TMD should undergo a TMJ imaging, especially when a diagnosis of DJD is proposed. There is no clear association between condyle morphology and DJD.[6] Furthermore, there is no statistical association between TMJ pain intensity and the severity of condylar resorption.[7]
The RDC/TMD has an examination protocol that suggests three types of images: pantomograph, MRI and CT/CBCT. Using the RDC/TMD as a reference standard, Ahmad et al. found that while CT images detected 75% of OA, MRI detected 40% and panoramic radiographs 0%.10 The use of CT/CBCT was thought to be the gold standard of imaging to evaluate DJD.5, 11 According to RDC/TMD, DJD is present when there is a gross crackling sound in the ATM. If it is accompanied by self-report of pain in the TMJ region and during palpation it is considered as diagnosis IIIb, osteoarthritis. Otherwise, no TMJ pain is present, diagnosis IIIc, of osteoarthritis is considered.
According to the DC/TMD, DJD is present when there is a self-assessment during the consultation or a history of TMJ noise, and test results show crepitus during maximum active open, passive open, right lateral, left lateral, or protrusive detected by the examiner.
There is no systematic review in the literature that addresses the topic mentioned in vivo, which highlights the importance of this section of Masticationpedia to understand how correct or limiting it is to make a diagnosis through imaging (CT, Cone beam, MNR, etc.) in a multifactorial functional pain manifestation. (Figures 1-4)

Figure 1: Polytomography of TMJ with closed mouth
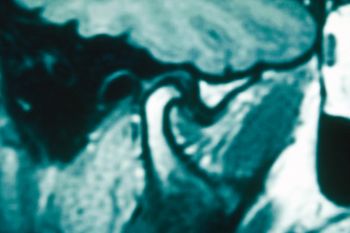
Figure 2: MRI, sagittal view of the ATM

Figure 3: MRI, frontal view of the TMJ

Figure 5: CT of the temporomandibular joints




The specific question is as follows:
Interpretation of TMJ imaging requires an understanding of normal joint anatomy.
As well described in the article by Seyed Mohammad Gharavi et al.[8] the TMJ is a synovial joint between the glenoid fossa of the temporal bone and the mandibular condyle. The central anatomical structure of the TMJ is the articular disc or meniscus. The disc is an oval-shaped fibrocartilaginous structure composed of anterior and posterior articular bands and a thinner center, called the intermediate zone. The intermediate zone gives the disc a biconcave appearance in the sagittal view. The posterior band is generally thicker than the anterior band and both bands are wider in the transverse dimension than in the anteroposterior dimension. The retrodisc tissue or bilaminar zone is rich neurovascular tissue that serves as the posterior attachment of the disc, fusing the disc with the joint capsule and temporal bone. (Figure 5)

{kind=link}
The lateral aspect of the disc connects with the joint capsule and inserts into the condylar neck. Anteriorly, the disc insertions are variable and called the "disc-capsular complex". The lateral pterygoid muscle fibers and tendons attach the anterior fascia of the disc to this complex. The position of the disc is assessed by the position of the posterior band and the intermediate zone with respect to the mandibular condyle.
The ATM has two compartments that work like two small joints within the same capsule. This allows for more range of motion relative to the size of the joint. The superior compartment separates the glenoid fossa of the temporal bone from the disc, while the inferior compartment separates the disc from the mandibular condyle. In the initial stage of mouth opening, the condyle rotates in the inferior articular compartment. It then translates anteriorly into the upper compartment.[9] The lateral pterygoid muscle helps open the jaw, and the medial pterygoid, masseter, and temporal muscles help close the jaw. As the condyle translates anteriorly, the disc should move between the condyle and the articular eminence. A normal disc does not move in the coronal plane during mouth opening.
- ↑ Priscila Brenner Hilgenberg-Sydney,1 Danielle Veiga Bonotto, José Stechman-Neto, Liete Figueiredo Zwir,3Camila Pachêco-Pereira, Graziela De Luca Canto, and André Luís Porporatti. Diagnostic validity of CT to assess degenerative temporomandibular joint disease: a systematic review. Dentomaxillofac Radiol. 2018 Jul; 47(5): 20170389. Published online 2018 Mar 2. doi: 10.1259/dmfr.20170389 PMCID: PMC6196046 PMID: 29480019
- ↑ de Leeuw R, Klasser GD. Orofacial pain: guidelines for assessment, diagnosis and management. 5th ed Hanover Park, IL: The British Institute of Radiology.; 2013. 312.
- ↑ Dworkin SF, LeResche L. Research diagnostic criteria for temporomandibular disorders: review, criteria, examinations and specifications, critique. J Craniomandib Disord 1992; 6: 301–55.
- ↑ Petersson A. What you can and cannot see in TMJ imaging-an overview related to the RDC/TMD diagnostic system. J Oral Rehabil2010; 37: 771–8. doi: 10.1111/j.1365-2842.2010.02108.x
- ↑ Bag AK, Gaddikeri S, Singhal A, Hardin S, Tran BD, Medina JA, et al.. Imaging of the temporomandibular joint: an update. World J Radiol 2014; 6: 567–82. doi: 10.4329/wjr.v6.i8.567
- ↑ Cömert Kiliç S, Kiliç N, Sümbüllü MA. Temporomandibular joint osteoarthritis: cone beam computed tomography findings, clinical features, and correlations. Int J Oral Maxillofac Surg 2015; 44: 1268–74. doi: 10.1016/j.ijom.2015.06.023
- ↑ Cevidanes LH, Hajati AK, Paniagua B, Lim PF, Walker DG, Palconet G, et al.. Quantification of condylar resorption in temporomandibular joint osteoarthritis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010; 110: 110–7. doi: 10.1016/j.tripleo.2010.01.008
- ↑ Seyed Mohammad Gharavi, Yujie Qiao, Armaghan Faghihimehr, and Josephina Vossen. Imaging of the Temporomandibular Joint. Diagnostics (Basel). 2022 Apr; 12(4): 1006. Published online 2022 Apr 16. doi: 10.3390/diagnostics12041006. PMCID: PMC9031630. PMID: 35454054
- ↑ Som P.M., Curtin H.D. Head and Neck Imaging—2 Volume Set. Mosby Elsevier; Maryland Heights, MO, USA: 2011. Expert Consult—Online and Print.